For several decades Dr. George J. Goodheart, Jr. produced Monthly AK Research Tapes -- LOADED with exceptional insights for the holistic physician. Here are the "Highlights" of Tape 4, Side 1 -- (with a few "illustrative pictures")
"Challenge of Cranial Faults
...

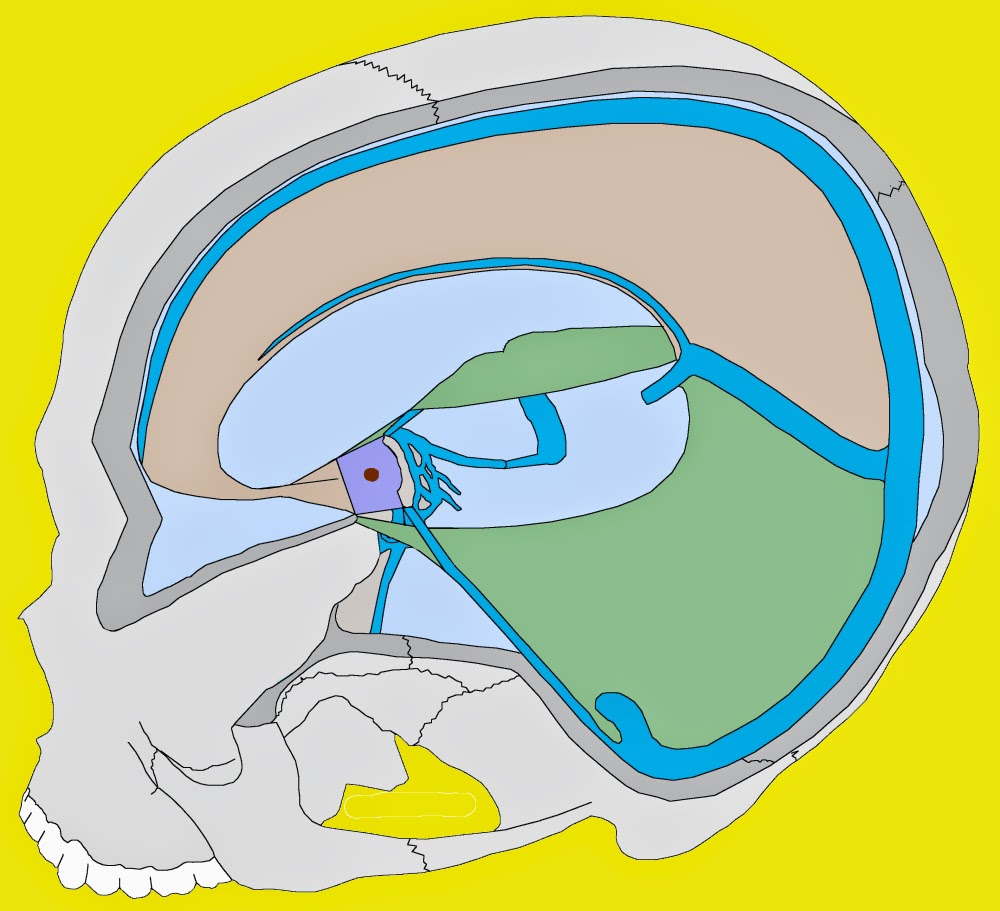
B. Internal frontal bone signs.
1. Wide nares on one side.
2. Narrow orbit on other side.
3. Super orbital notch soreness.
C. External frontal signs.
1. Wide orbit
2. Painful eyeball on wide orbit side.
3. Painful cheek bone on opposite side.
D. These external signs may be present without anterior neck flexor weakness.
E. Procedure for challenging internal frontal. Example: Wide nares, narrow orbit side.


1. Patient is in supine position.
2. Put pressure on malar bone.
3. Press medially toward base of nose with 4 or 5 lbs. pressure.
4. If there is a partial internal frontal bone rotation, the anterior neck flexors will show strength, but when pressure is applied to the malar bone as described above, this will cause an immediate weakness of the anterior neck flexors.
F. Correct internal frontal bone in usual way.
1. Go to side of wide nares, narrow orbit using roll out type pressure on the alveolar process.
2. Go past teeth into pterygoid pocket and press footward.
3. Get on pterygoid process on the opposite side of press upward.
G. Re-challenge malar arch and anterior neck flexors will not blow.
H. External frontal bone rotation.
1. Wide orbit with no change in nares.
2. The wide orbit side has painful eyeball.
3. Narrow orbit side has painful cheek bone.
I. External frontal bone challenge.

1. Go to narrow orbit side.
2. Grasp upper molar teeth and pulls downward with 4 or 5 lbs. pressure, (if the patient has dentures, try to grasp gums in that area).
3. Retest anterior neck flexors.
4. If partial external frontal bone rotation, flexors will go weak.
5. Correct external frontal bone as follows:
a. Press lateral to cruciate ligament on hard palate on narrow orbit side, press toward vertex of skull.
b. Check eyeball pain, pressing on cruciate ligament in direction that eliminates it.




J. Use in difficult cervical and whiplash injuries."


"Challenge of Cranial Faults
...
A. Sign of internal or external rotated frontal is weakness of anterior neck flexors.
B. Internal frontal bone signs.
1. Wide nares on one side.
2. Narrow orbit on other side.
3. Super orbital notch soreness.
C. External frontal signs.
1. Wide orbit
2. Painful eyeball on wide orbit side.
3. Painful cheek bone on opposite side.
D. These external signs may be present without anterior neck flexor weakness.
E. Procedure for challenging internal frontal. Example: Wide nares, narrow orbit side.
1. Patient is in supine position.
2. Put pressure on malar bone.
3. Press medially toward base of nose with 4 or 5 lbs. pressure.
4. If there is a partial internal frontal bone rotation, the anterior neck flexors will show strength, but when pressure is applied to the malar bone as described above, this will cause an immediate weakness of the anterior neck flexors.
F. Correct internal frontal bone in usual way.
1. Go to side of wide nares, narrow orbit using roll out type pressure on the alveolar process.
2. Go past teeth into pterygoid pocket and press footward.
3. Get on pterygoid process on the opposite side of press upward.
G. Re-challenge malar arch and anterior neck flexors will not blow.
H. External frontal bone rotation.
1. Wide orbit with no change in nares.
2. The wide orbit side has painful eyeball.
3. Narrow orbit side has painful cheek bone.
I. External frontal bone challenge.
1. Go to narrow orbit side.
2. Grasp upper molar teeth and pulls downward with 4 or 5 lbs. pressure, (if the patient has dentures, try to grasp gums in that area).
3. Retest anterior neck flexors.
4. If partial external frontal bone rotation, flexors will go weak.
5. Correct external frontal bone as follows:
a. Press lateral to cruciate ligament on hard palate on narrow orbit side, press toward vertex of skull.
b. Check eyeball pain, pressing on cruciate ligament in direction that eliminates it.
J. Use in difficult cervical and whiplash injuries."